How much is too much?
In part one of “Exercise and the Heart” I reviewed the adaptations of the heart in response to training and exercise. While most regard these changes to be normal and physiologic, many have questioned whether extreme amounts of exercise may put athletes at higher risk for certain – and potentially life threatening – cardiac problems.
We know from studies of former athletes that athletes live longer, compared to the general population.1 But cases of sudden death in athletes, while rare, occur with enough frequency (and profound impact) that significant attention has been paid to better understand what contributes to these events, how we can prevent them in the future, and what role exercise/training/competition may play. Young athletes (<35 years) that die during competition typically have an inherited or congenital condition (like hypertrophic cardiomyopathy) which predisposes them to dangerous and lethal heart rhythms during exercise. In older athletes, death during competition is most commonly due to coronary artery disease, or narrowing of the heart arteries due to cholesterol build-up. When these diseases are diagnosed in athletes, we may recommend restriction and disqualification from competition. But what about athletes with “normal” hearts? Does prolonged training, competition, or extreme forms of exercise lead to downstream heart problems?
Several recent findings have brought these questions to the forefront. Athletes, particularly endurance athletes, seem to be more likely to have calcification of their coronary arteries – indicative of coronary artery disease.2 There is still much to learn from this standpoint, as others have shown that although more calcium is present, it may represent cholesterol plaques that are actually more stable, and less likely to cause a heart attack.3 We have also found small areas of scar within the hearts of some, otherwise healthy athletes, which may be due to repetitive micro-injury to heart muscle during extreme bouts of exercise – this may put athletes at a greater risk of dangerous or deadly heart rhythms.4
Despite these potentially negative associations with extreme and/or prolonged exercise, the primary question is: do these findings matter? Do they lead to clinical events, such as sudden or premature death, or heart attacks, etc.? We know that exercise decreases mortality, but does the risk of death flatten out, or even start to go back up with extreme amounts of exercise? Some have suggested a U-shaped relationship between exercise and “cardiac events”, where no exercise poses a high risk, moderate amounts of exercise lead to a reduction in risk, but at a certain upper threshold of exercise, that risk starts to increase again.5
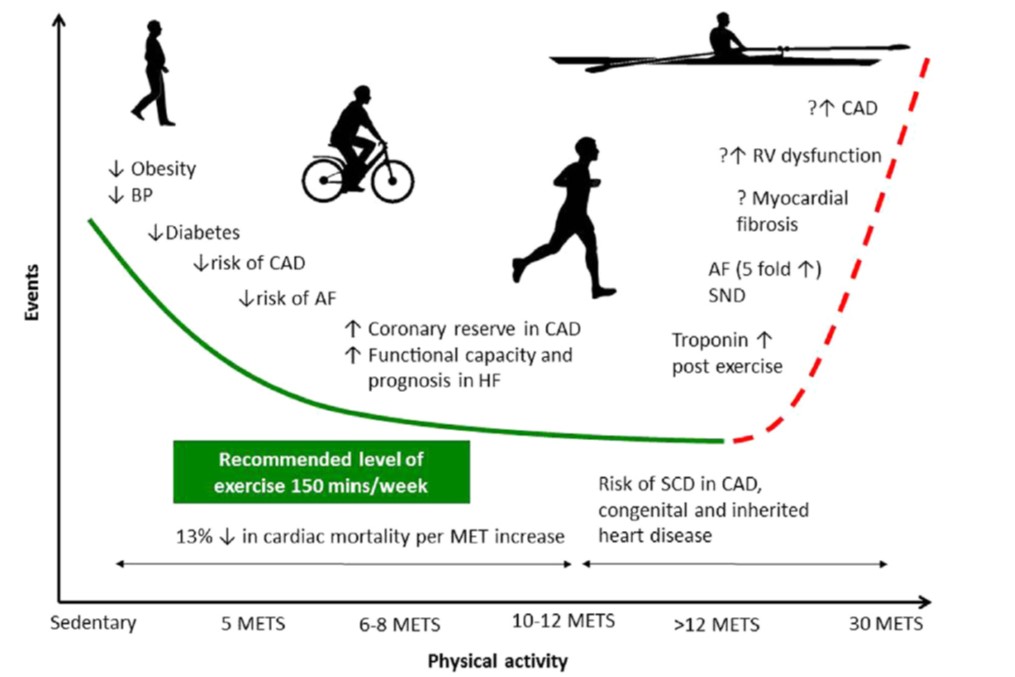
Proposed U-shaped relationship between activity and cardiovascular events. METS = metabolic equivalents, which is a standard unit of aerobic work (1 MET = 3.5 mL/kg/min O2 consumption).
Figure from Merghani A, Malhotra A, Sharma S. Trends in Cardiovascular Medicine, 2016
This question has been studied using self-reported exercise data – specifically in runners6,7, as well as in the general population8. These studies seem to support the notion that extreme amounts of exercise, while overall beneficial compared to sedentary individuals, did not continue to provide additional benefit after some threshold amount. In other words, there was a plateau of benefit once a certain amount of exercise per week was performed. In one study of runners, from the Copenhagen City Heart Study, they actually found that the runners who ran the most actually died more frequently than those who ran a modest amount, suggesting that high running volumes may cause net harm. A primary limitation of these studies is that self-reported exercise data is exactly that: self-reported. As it turns out, people aren’t particularly reliable or accurate at assessing their own exercise habits. This leads to biased and potentially inaccurate data.
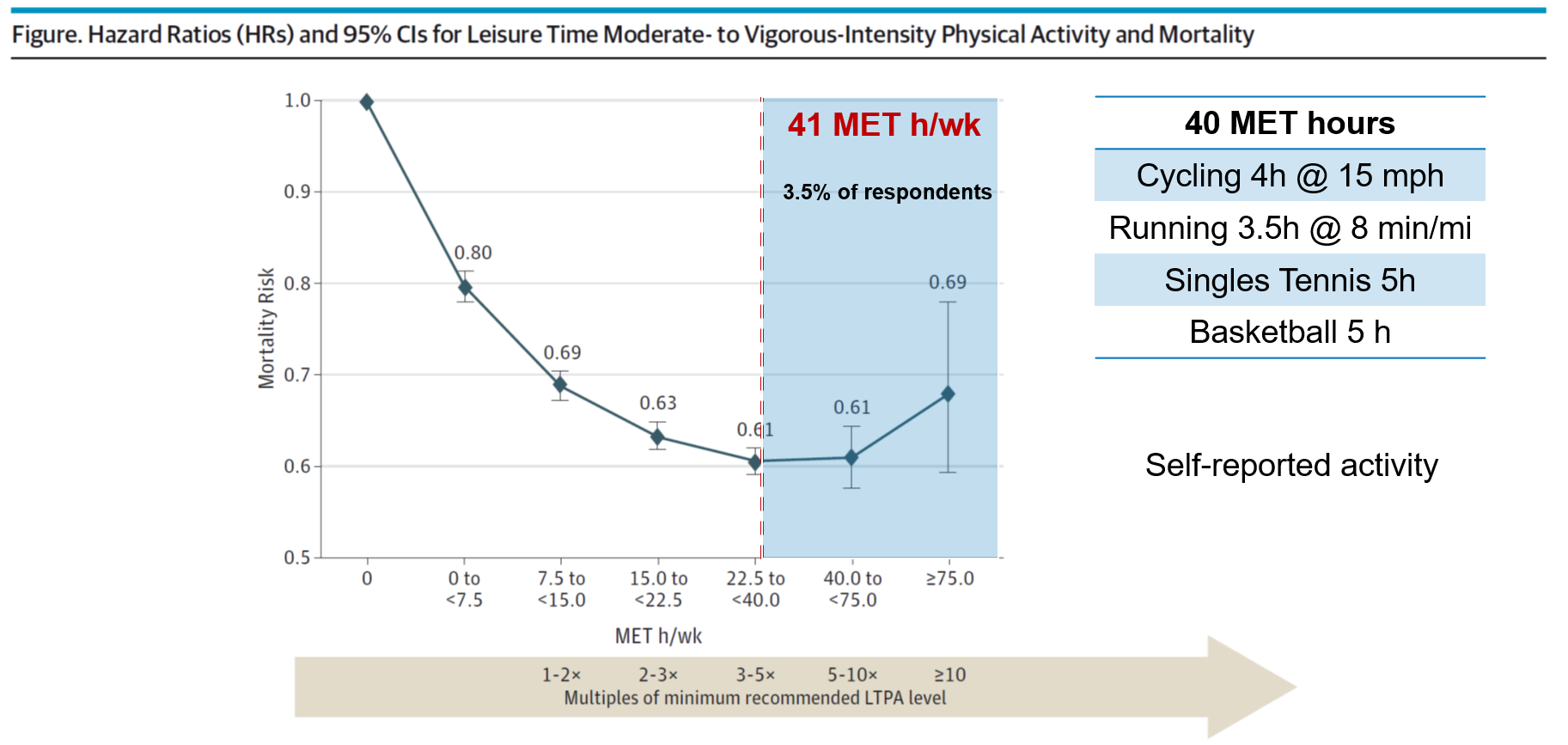
A plateau or U-shaped relationship between self-reported activity level and mortality risk, with peak “benefit” at 41 MET hours/week. Examples of activity equivalent to 40 MET hours on the right.
Figure adapted from Arem H, Moore SC, Patel A, et al. JAMA Intern Med, 2015
Myself and other researchers at the Cleveland Clinic recently asked whether we could better understand the mortality risk of very active individuals (at the far right of these curves) by using objectively measured aerobic fitness. We analyzed data from >122,000 patients who underwent exercise treadmill testing from 1990-2014, and grouped patients into performance categories by age and gender. We then used statistical modeling to account for baseline differences, including things like age, gender, tobacco use and BMI, as well as a number of clinical comorbidities including coronary disease, hypertension, diabetes, etc. The results of our study were recently published in the Journal of the American Medical Association (JAMA) , and have generated some press. I would encourage anyone that’s interested to read the original article – but I wanted to provide a synopsis of our study and findings, and my own take on the results.
Performance was measured as peak achieved METS (a standard estimation of aerobic work) and groups were defined by percentiles: Low (<25th), Below Average (25-49th), Above Average (50-74th), High (75-97.6th), and Elite (≥97.7th). Elite performers showed aerobic fitness roughly comparable to those of endurance athletes. I’ve provided the table with specific group cut-offs below, for those interested or that want to see what group they might be in (you can roughly estimate your peak METS using a prior running race result and one of several online VO2Max predictors/calculators; just divide your estimated VO2max by 3.5 to convert to METS)
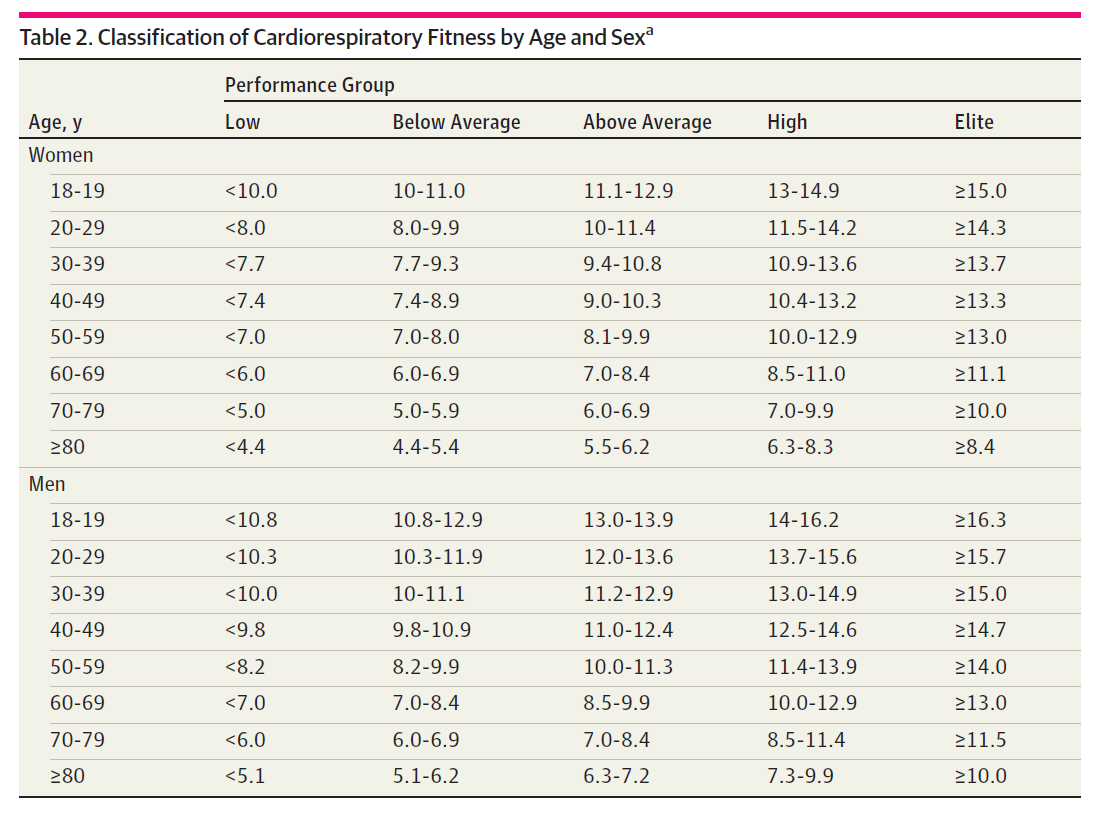
From Mandsager, et al (JAMA Open Network, 2018).
What we found was that with each step up in aerobic fitness, the risk of death decreased. Even when compared to high performers, extremely fit patients (“elite” performers) showed additional survival benefit. There was no evidence of a plateau effect or U-shaped relationship – simply put, the fitter a patient was, the lower their risk of dying. We found no upper limit of benefit to aerobic fitness.
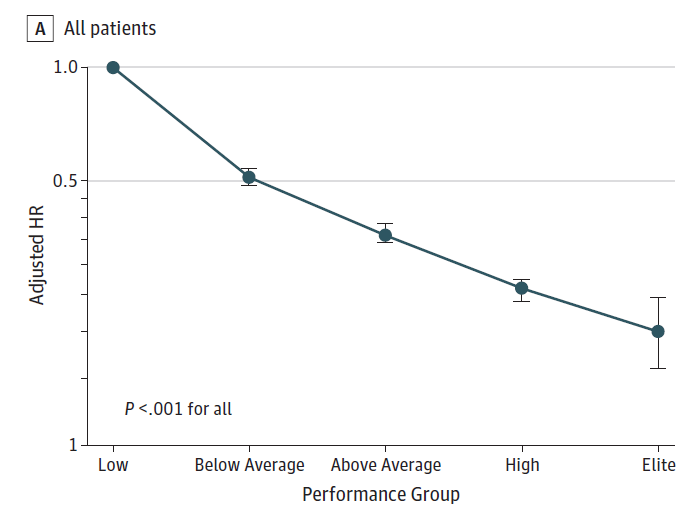
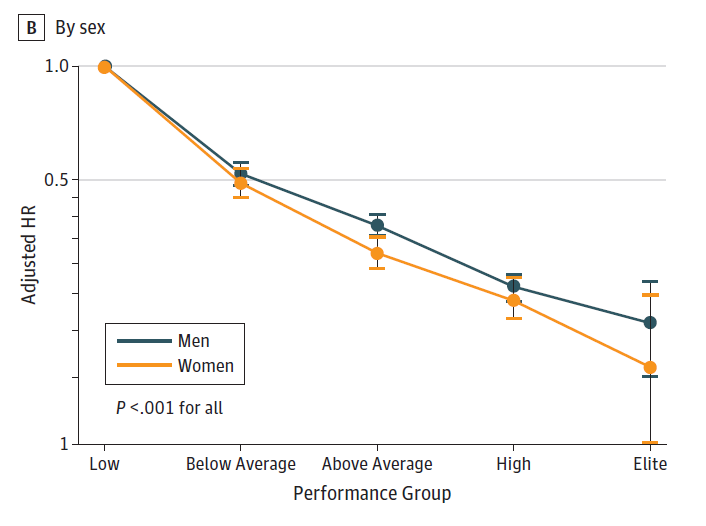
Relationship between mortality risk (y-axis) and aerobic fitness (by performance group; x-axis), relative to the lowest performers.
From Mandsager, et al (JAMA Open Network, 2018)
It is important to acknowledge the limitations of these findings. The most important is that this is an observational study – we didn’t randomize people to more or less exercise – so just because fitness is correlated with survival, we cannot say that fitness caused people to live longer (though in the context of a large body of evidence on the benefits of exercise and fitness, I think it’s reasonable to conclude that fitness played a role). These are also individuals referred for medical stress testing, and not a sample of the general population – so this referral bias may influence our findings. Lastly, we are measuring aerobic fitness – not exercise, per se, though exercise is the primary component of one’s fitness (genetics may make up 20-30%).
But our findings are consistent with a large body of evidence looking at the health and life-expectancy of ex-athletes, which very clearly and consistently has shown that these athlete’s live longer. When you look at objective (not self-reported) measurements of fitness, we see no signal that extremely high fitness puts patients at additional risk – in fact it continues to be associated with a lower risk of death, even when compared to more modestly fit individuals.
While more work needs to be done on the effects of extreme exercise, our findings should at least put the benefits and potential risks into perspective. We should all be encouraged to get fit (or get fitter!) – and for those of you who enjoy pushing yourself to your aerobic limit, keep at it!
Disclaimer: These data are from a large population – individual circumstances may change the benefits/risks of vigorous exercise. Make sure to check with your doctor before starting a new exercise regimen, especially if you have a known health condition, or if you are having new or concerning symptoms with exercise.
References
1. Lemez S, Baker J. Do Elite Athletes Live Longer? A Systematic Review of Mortality and Longevity in Elite Athletes. Sports Med – Open [Internet]. 2015 [cited 2016 Jul 6];1. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4534511/
2. Merghani A, Maestrini V, Rosmini S, Cox AT, Dhutia H, Bastiaenan R, David S, Yeo TJ, Narain R, Malhotra A, Papadakis M, Wilson MG, Tome M, AlFakih K, Moon JC, Sharma S. Prevalence of Subclinical Coronary Artery Disease in Masters Endurance Athletes With a Low Atherosclerotic Risk Profile. Circulation [Internet]. 2017 [cited 2018 Oct 31];Available from: http://www.ahajournals.org/doi/abs/10.1161/circulationaha.116.026964
3. AengevaerenVL, Mosterd A, Braber TL, Prakken NHJ, Doevendans PA, Grobbee DE, Thompson PD,Eijsvogels TMH, Velthuis BK. The Relationship Between Lifelong Exercise Volumeand Coronary Atherosclerosis in Athletes. Circulation [Internet]. 2017
;CIRCULATIONAHA.117.027834. Available from: http://circ.ahajournals.org/content/early/2017/04/27/CIRCULATIONAHA.117.027834
4. van de Schoor FR, Aengevaeren VL, Hopman MTE, Oxborough DL, George KP, Thompson PD, Eijsvogels TMH. Myocardial Fibrosis in Athletes. Mayo Clin Proc. 2016;91:1617–1631.
5. Merghani A, Malhotra A, Sharma S. The U-shaped relationship between exercise and cardiac morbidity. Trends Cardiovasc Med [Internet]. 2016;26:232–240. Available from: http://www.sciencedirect.com/science/article/pii/S1050173815001711
6. Lee D, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-Time Running Reduces All-Cause and Cardiovascular Mortality Risk. J Am Coll Cardiol [Internet]. 2014 [cited 2018 May 18];64:472–481. Available from: http://www.sciencedirect.com/science/article/pii/S0735109714027466
7. Schnohr P, O’Keefe JH, Marott JL, Lange P, Jensen GB. Dose of Jogging and Long-Term Mortality: The Copenhagen City Heart Study. J Am Coll Cardiol [Internet]. 2015 [cited 2018 Apr 9];65:411–419. Available from: http://www.sciencedirect.com/science/article/pii/S0735109714071745
8. Arem H, Moore SC, Patel A, Hartge P, Gonzalez AB de, Visvanathan K, Campbell PT, Freedman M, Weiderpass E, Adami HO, Linet MS, Lee I-M, Matthews CE. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern Med [Internet]. 2015 [cited 2018 Apr 25];175:959–967. Available from: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2212267